
MCL Injury
An MCL injury, or medial collateral ligament injury, is one of the most prevalent knee injuries, primarily affecting the inner aspect of the knee.
The MCL extends from the femur (thigh bone) to the tibia (shin bone) and is positioned on the inner side of the knee joint. Comprising three main anatomic structures, the medial knee structures include the robust superficial medial collateral ligament, along with the posterior oblique and deep medial collateral ligaments. It’s essential to understand that an MCL injury involves damage to the entire medial knee structures.
Typically, isolated MCL injuries occur due to sporting activities. These injuries can result from external force applied to the outside of the knee, leading to stretching or tearing of the medial knee structures. Such injury mechanisms can occur either through direct contact or non-contact incidents.
Symptoms of an MCL tear may include:
To accurately diagnose an MCL injury, Dr. Ravi Teja Rudraraju conducts a thorough examination using x-rays, stress x-rays, and occasionally MRI scans to assess the MCL area and determine the extent of the injury. An MRI is particularly useful for identifying whether the injury is a partial or complete tear of the MCL and which specific parts of the medial knee structures are affected.
Dr. Ravi Teja Rudraraju may perform a valgus stress test during the examination. This test involves applying lateral force to the knee while it is both straight and flexed to 30° to evaluate side-to-side gapping, indicative of an MCL tear. This test, along with other physical examinations, aids in the accurate diagnosis of MCL injuries. For comprehensive evaluation and management of MCL injuries, individuals can seek assistance from Dr. Ravi Teja Rudraraju at https://drraviteja.com.
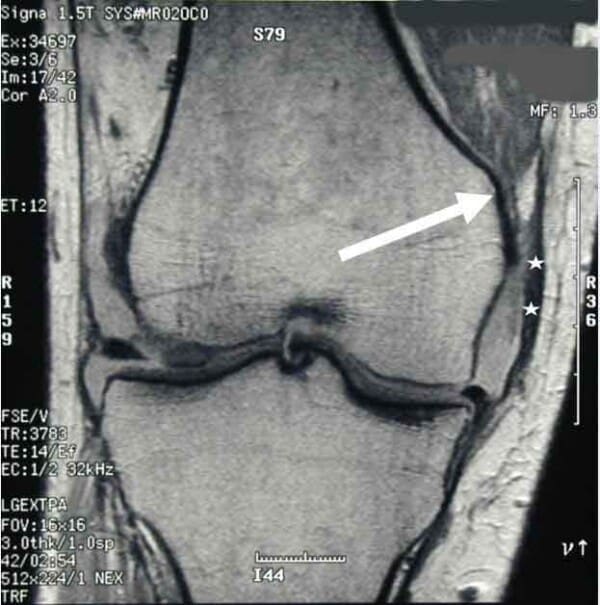
An MRI scan reveals a tear of the medial collateral ligament (MCL) detached from the femur. Tears occurring at the femur attachment site, particularly in cases where the knee does not exhibit side-to-side gapping when tested in full extension, demonstrate a higher likelihood of healing compared to MCL tears at the tibia attachment site. For further evaluation and personalized treatment options, individuals can consult Dr. Ravi Teja Rudraraju at https://drraviteja.com.
MCL Tear Symptoms:
To diagnose an MCL injury accurately, Dr. Ravi Teja Rudraraju conducts a thorough examination, including x-rays, stress x-rays, and occasionally, an MRI. MRI scans provide detailed images of ligaments, muscles, and bones, aiding in determining the extent of the MCL injury, whether partial or complete, and which structures of the medial knee are affected.
A valgus stress test is performed by Dr. Ravi Teja Rudraraju to assess the integrity of the MCL. This test involves applying side-to-side pressure to the knee with the leg straight and flexed at 30°. Increased gapping during this test indicates a likely MCL tear.
MCL Injury Grading:
Most acute Grade I and II injuries can heal with proper rehabilitation. However, close monitoring is necessary for Grade III injuries to ensure there are no residual instability issues. In cases of combined knee ligament injuries, particularly with a concurrent PCL tear, concurrent repair, augmentation repair, or complete medial knee reconstruction may be necessary to prevent ACL graft failure. For expert evaluation and treatment of MCL injuries, individuals can consult Dr. Ravi Teja Rudraraju at https://drraviteja.com.
When is MCL Surgery Needed?
Traditionally, surgical intervention for medial knee injuries posed a risk of postoperative stiffness for patients, often leading to additional surgeries. To mitigate this, our research laboratory has developed advanced techniques aimed at promoting early knee movement, thus reducing the likelihood of stiffness and the need for secondary procedures.
Dr. Ravi Teja Rudraraju has conducted extensive research into the anatomy, biomechanics, and diagnosis of medial knee structures. This research has led to the development of an innovative anatomic medial knee reconstruction procedure, which is currently undergoing clinical outcome studies.
What is MCL Surgery Recovery Time?
In cases of acute medial knee ligament tears, patients are fitted with a brace and begin an early rehabilitation program focusing on quadriceps reactivation, edema control, and knee range of motion. Stationary biking is a primary rehabilitation exercise for MCL tears.
For isolated acute MCL injuries, athletes can generally return to sports within a timeframe determined by multiplying the injury grade by two (in weeks). For instance, a grade I acute MCL injury typically requires 1-2 weeks to heal, while a grade II injury may take 3-4 weeks. A complete grade III MCL injury usually necessitates 5-6 weeks of guided rehabilitation for complete healing.
In cases of significant knee instability, the use of a hinged MCL protective knee brace is often recommended during the acute phase. Patients can be fitted with the brace by our specialists to ensure proper fit and durability for their activity levels. For expert guidance on MCL injuries and their management, individuals can visit https://drraviteja.com and consult with Dr. Ravi Teja Rudraraju.
Have you sustained an MCL injury?
There are two ways to initiate a consultation with Dr. Ravi Teja Rudraraju
You can provide current X-rays and/or MRIs for a clinical case review with with Dr. Ravi Teja Rudraraju
You can schedule an office consultation with Dr. Ravi Teja Rudraraju
Frequently Asked Questions
Many MCL injuries have the potential to heal, especially if the MCL is the sole ligament affected around the knee. Partial MCL tears almost invariably heal, while complete tears of the MCL mostly heal. However, MCL tears that occur alongside other ligament injuries in the knee, particularly with the PCL, have a lower likelihood of healing completely. Complete MCL tears that detach from the femur or the tibia typically do not heal.
The pain associated with an MCL tear can vary depending on the severity of the injury. Pain is often due to bleeding and swelling from the injury. While minor MCL sprains may not cause significant pain, most complete tears result in pain, particularly when pressure is applied to the injured area. Individuals with a history of MCL tears may not experience much pain if the ligament previously healed in a slightly loose manner.
In most cases, an ACL tear is considered a more severe injury than an MCL tear. This is because an ACL tear occurs within the joint, where the healing environment is poor, whereas the MCL tear typically has a better chance of healing due to its good blood supply. Moreover, MCL reconstructions have a higher success rate than ACL reconstructions.
An MCL injury results from excessive stress on the inside of the knee, causing the fibers within the ligament to stretch. This can occur due to a variety of factors, including a direct blow to the outside of the knee, falling toward the inside of the knee, or significant twisting motions during sports activities.
Testing for an MCL injury involves palpation and stress testing to assess the extent of the tear. Palpation over the medial knee area may reveal pain, swelling, or thickening indicative of an MCL tear. Stressing the knee through valgus stress tests can determine the severity of the tear, with grade I, II, and III injuries characterized by varying degrees of gapping and instability.
Most MCL tears heal, particularly when they occur in isolation without concurrent ligament injuries. Initial steps in treatment involve reducing swelling and bleeding to facilitate knee motion and normal gait. Utilizing a hinged knee brace can help stabilize the knee during the healing process. Additionally, early knee motion exercises, such as stationary biking, promote proper alignment of MCL collagen fibers, leading to faster healing. The duration of recovery varies depending on the severity of the tear, with grade I tears typically healing in 1-2 weeks, grade II tears in 3-4 weeks, and grade III tears in 5-7 weeks.
While less common, an MCL tear can occur from running, particularly if there is a sudden twisting or jolting movement that places stress on the inside of the knee.
Yes, skiing is a common cause of MCL tears due to the mechanics involved, especially during falls or slips that cause the knee to collapse inward. MCL tears frequently co-occur with ACL tears in skiers.
When an individual with an MCL tear cannot fully straighten their leg, it may indicate additional injuries within the knee, such as a torn ACL or meniscal tear. Pain and swelling may also contribute to difficulty in knee extension, which can be addressed through rehabilitation to reduce swelling and improve knee motion.
MCL injuries in soccer or football often result from external forces causing stress on the inside of the knee. Rehabilitation typically involves a combination of icing, bracing, and stationary biking to enhance range of motion and quadriceps strength, with return to activity contingent upon the severity of the injury.
For expert guidance on MCL injuries and their management, individuals can visit https://drraviteja.com and consult with Dr. Ravi Teja Rudraraju.